
Hepatitis B management has become more precise over the past two decades, largely because clinicians can now measure viral activity directly rather than relying on indirect markers alone. The ability to quantify viral load in a patient’s blood has changed how treatment decisions are made, how therapy response is monitored, and how disease progression is assessed. Yet the gap between what clinical guidelines expect from viral load testing and what laboratories consistently provide remains a practical concern for hepatologists, infectious disease specialists, and laboratory directors alike.
Guidelines from major hepatology bodies are built on assumptions about assay performance, standardization, and inter-laboratory consistency. Those assumptions are not always met in real clinical environments. Understanding where the gap exists, why it exists, and what it means for patient care requires looking at the standards themselves alongside how testing actually performs across different laboratory settings.
The Clinical Standard for HBV DNA Measurement and Why Consistency Matters
The role of HBV DNA PCR quantitative testing in hepatitis B management is not supplementary — it is central. Both the American Association for the Study of Liver Diseases (AASLD) and the World Health Organization (WHO) have embedded viral load quantification into the core logic of their clinical frameworks. Treatment initiation thresholds, antiviral monitoring intervals, and endpoints for considering therapy discontinuation are all tied to specific viral load reference points that only a reliable quantitative PCR assay can define.
The WHO established an International Standard for HBV DNA to address one of the earliest and most persistent problems in viral load testing: results from different laboratories were not comparable. A patient tested at one facility could receive a meaningfully different result than if tested at another, even when the actual viral burden was identical. The international unit per milliliter (IU/mL) was adopted as the standardized reporting unit precisely to resolve this. However, adopting a standard reporting unit does not automatically mean every laboratory’s assay performs to the same level of sensitivity, linearity, or reproducibility.
What Guidelines Expect from an HBV DNA Assay
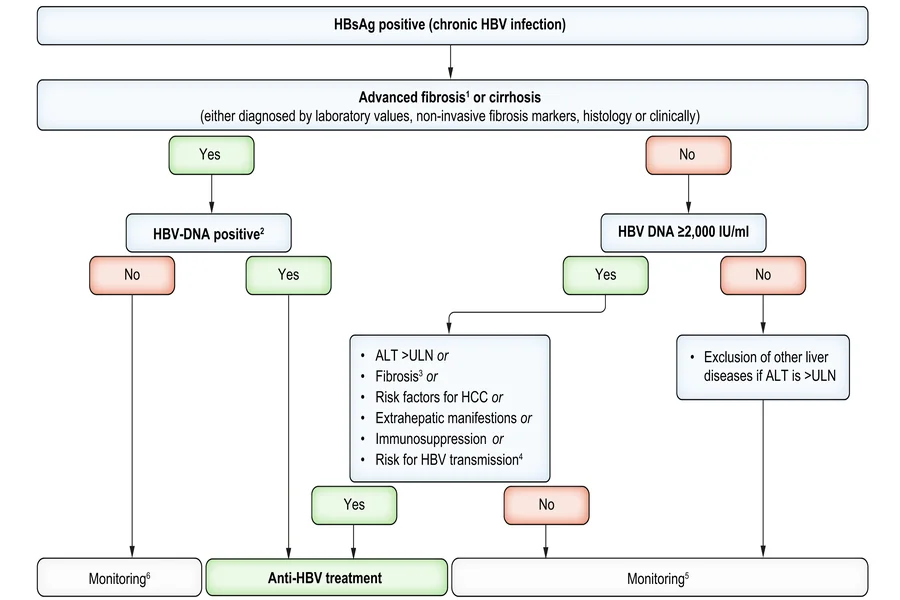
AASLD guidelines for chronic hepatitis B describe viral load thresholds that inform some of the most consequential clinical decisions a hepatologist makes. When viral load is undetectable or below a certain threshold in a patient with HBeAg-negative disease, treatment may not be indicated. When it rises above a defined level in a patient with cirrhosis, the urgency of treatment changes. These decisions depend entirely on the assay being able to detect, quantify, and accurately report viral DNA within a clinically meaningful range.
Guidelines generally assume that the assay in use can detect HBV DNA at low concentrations without losing accuracy, that it performs consistently across the range of clinical relevance, and that results are reproducible over time within the same laboratory. These are reasonable expectations, but they translate into specific technical demands that not every laboratory fulfills equally.
The WHO International Standard and Its Intended Function
The WHO International Standard for HBV DNA, maintained and updated periodically, gives manufacturers and laboratories a reference point against which their assays can be calibrated. When a laboratory reports a result in IU/mL that is traceable to this standard, the implication is that results can be compared across platforms and over time. According to the WHO Expert Committee on Biological Standardization, this standardization process is designed to reduce the systematic variation that historically made viral load testing unreliable as a consistent clinical tool.
The problem is that traceability to the international standard does not guarantee performance at the low end of detection, where many of the most clinically significant decisions are made. A patient near the lower limit of quantification may receive different management advice depending on which laboratory processed the sample and which platform was used.
Where Laboratory Performance Diverges from Guideline Assumptions
Clinical guidelines are written at the level of principle, not platform specification. They describe what a clinician should do when viral load is undetectable, low, or elevated — but they do not, and arguably cannot, account for the variation in how different laboratories achieve those measurements. The consequence is that the same guideline can produce different clinical outcomes depending on where testing is performed.
Several areas of divergence are well documented in the laboratory medicine literature. Sensitivity at the lower limit of quantification varies across commercial platforms. The dynamic range over which an assay remains accurate is not uniform. Inhibition from complex sample matrices, particularly in patients with certain comorbidities or abnormal plasma components, can affect result accuracy. And in settings where testing is outsourced or processed in batches, turnaround time may not align with the clinical urgency that guidelines implicitly assume.
Lower Limit of Detection vs. Lower Limit of Quantification
These two concepts are often treated as interchangeable in clinical practice, but they represent distinct analytical boundaries. The lower limit of detection refers to the lowest concentration at which a signal is reliably distinguished from background noise. The lower limit of quantification is the lowest concentration at which the assay can assign an accurate numeric value. Results that fall between these two thresholds are typically reported as “detected but below the limit of quantification,” which presents a real challenge for clinicians applying guideline thresholds.
When a guideline describes “undetectable” viral load as a marker of treatment response or a condition for considering therapy cessation, the clinical meaning of that term depends on the assay’s specific limits. A result reported as undetectable on one platform may represent a meaningful viral burden on another with lower sensitivity. This is not a hypothetical concern — it affects treatment monitoring in a practical and recurring way.
Platform Variability and the Problem of Serial Monitoring
Monitoring a patient’s viral load over time requires more than accurate single-point measurement. It requires that the results across multiple time points are comparable, which means either using the same platform consistently or accounting for known inter-platform differences. In practice, many patients receive care across different facilities, and laboratory platforms change due to procurement cycles, contract switches, or technical transitions.
When the platform changes mid-monitoring, a clinician may observe what appears to be a meaningful shift in viral load — an increase or decrease that triggers a clinical decision — when the change is actually an artifact of inter-platform variation rather than a true biological change. Guidelines do not provide clear direction on how to handle these transitions, leaving clinicians to interpret ambiguous data without formal methodological support.
The Operational Reality for Laboratories Running HBV DNA Testing
For laboratory directors and clinical pathologists, the challenge of HBV DNA quantification is not simply a matter of selecting a validated assay and running it. It involves managing quality control processes, participating in external proficiency testing programs, maintaining appropriate calibration against reference materials, and ensuring that result interpretation guidance communicates the assay’s limitations to ordering clinicians clearly.
External quality assessment programs, run by organizations such as the College of American Pathologists, reveal that inter-laboratory variability in HBV DNA quantification persists even among accredited facilities using well-validated commercial platforms. The degree of variation tends to be most pronounced at the extremes of the reportable range — the very points where clinical decisions are most sensitive.
Reporting Practices and Clinical Communication
How a laboratory reports an HBV DNA result is as important as the result itself. Reporting “less than the lower limit of quantification” without specifying what that limit is, or reporting in log units without providing guidance on clinical significance, can contribute to misinterpretation. Laboratories that provide clear result reports — including the method used, the reportable range, and contextual notes for borderline values — reduce the risk of clinical decision-making based on misread data.
This is an area where laboratory practice often falls short of the implicit expectations built into clinical guidelines. Guidelines assume the clinician receives a result with known, consistent properties. In reality, the result’s reliability depends on what happens between sample collection and result reporting, and that chain is not always transparent to the ordering physician.
Aligning Guideline Intent with Laboratory Capability
Closing the gap between what guidelines describe and what laboratories deliver requires action at multiple levels. It is not a problem that resolves itself through good intentions or general quality improvement language. It requires structured engagement between clinical and laboratory teams, clear criteria for assay selection, and ongoing attention to whether testing performance supports the clinical framework in which results are used.
Clinicians who understand the operational limits of hbv dna pcr quantitative testing are better equipped to interpret results correctly, request confirmatory testing when indicated, and avoid acting on apparent changes in viral load that may reflect measurement variability rather than disease activity. Laboratories that communicate their assay’s performance characteristics clearly, and that participate consistently in proficiency testing programs, provide the foundation that clinical decision-making actually requires.
- Selecting an assay with a well-characterized lower limit of quantification reduces ambiguity in low-viral-load monitoring scenarios.
- Maintaining platform consistency for individual patients across serial monitoring reduces the risk of misinterpreting inter-platform variability as clinical change.
- Structured laboratory reports that include assay-specific performance context give clinicians the information they need to apply guideline thresholds accurately.
- Participation in external quality assessment programs provides laboratories with ongoing data on how their results compare to peer facilities using similar and different platforms.
- Direct communication between hepatology and laboratory medicine teams, particularly when assay or platform changes are planned, reduces the clinical risk that transitions introduce.
Conclusion
The science behind hbv dna pcr quantitative testing has advanced considerably, and the clinical guidelines built on that science reflect genuine progress in understanding how viral load correlates with disease activity and treatment response. But guidelines are written for an ideal analytical environment, and the environment in which most testing occurs is more variable than guidelines can account for.
The practical reality is that the quality of a viral load result depends on decisions made at the laboratory level — assay selection, calibration, reporting practices, and quality oversight — as much as it depends on the guideline framework a clinician is applying. When those two layers are well aligned, hbv dna pcr quantitative testing delivers on its clinical promise. When they are not, the result is interpretive uncertainty that may not be visible to the clinician at the point of decision.
For hepatologists, infectious disease physicians, and laboratory professionals working in this space, understanding both layers is not optional. It is the foundation of responsible hepatitis B management. Guidelines set the direction. Laboratory performance determines whether that direction is actually achievable in practice.